Dengrong Jiang1,2, Zixuan Lin1,2, Peiying Liu1, Sandeepa Sur1, Cuimei Xu1, Kaisha Hazel1, George Pottanat1, Jacqueline Darrow3, Jay J. Pillai1,4, Sevil Yasar5, Paul Rosenberg6, Abhay Moghekar3, Marilyn Albert3, and Hanzhang Lu1,2,7
1The Russell H. Morgan Department of Radiology & Radiological Science, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 2Department of Biomedical Engineering, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 3Department of Neurology, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 4Department of Neurosurgery, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 5Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 6Department of Psychiatry and Behavioral Sciences, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 7F.M. Kirby Research Center for Functional Brain Imaging, Kennedy Krieger Research Institute, Baltimore, MD, United States
1The Russell H. Morgan Department of Radiology & Radiological Science, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 2Department of Biomedical Engineering, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 3Department of Neurology, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 4Department of Neurosurgery, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 5Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 6Department of Psychiatry and Behavioral Sciences, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 7F.M. Kirby Research Center for Functional Brain Imaging, Kennedy Krieger Research Institute, Baltimore, MD, United States
Cerebral oxygen extraction fraction (OEF) is
differentially affected by Alzheimer’s (decrease OEF) and vascular (increase
OEF) pathology. Therefore, OEF can be useful in differential diagnosis of
Alzheimer’s disease and vascular cognitive impairment.

Table 1. Characteristics of the
participants.
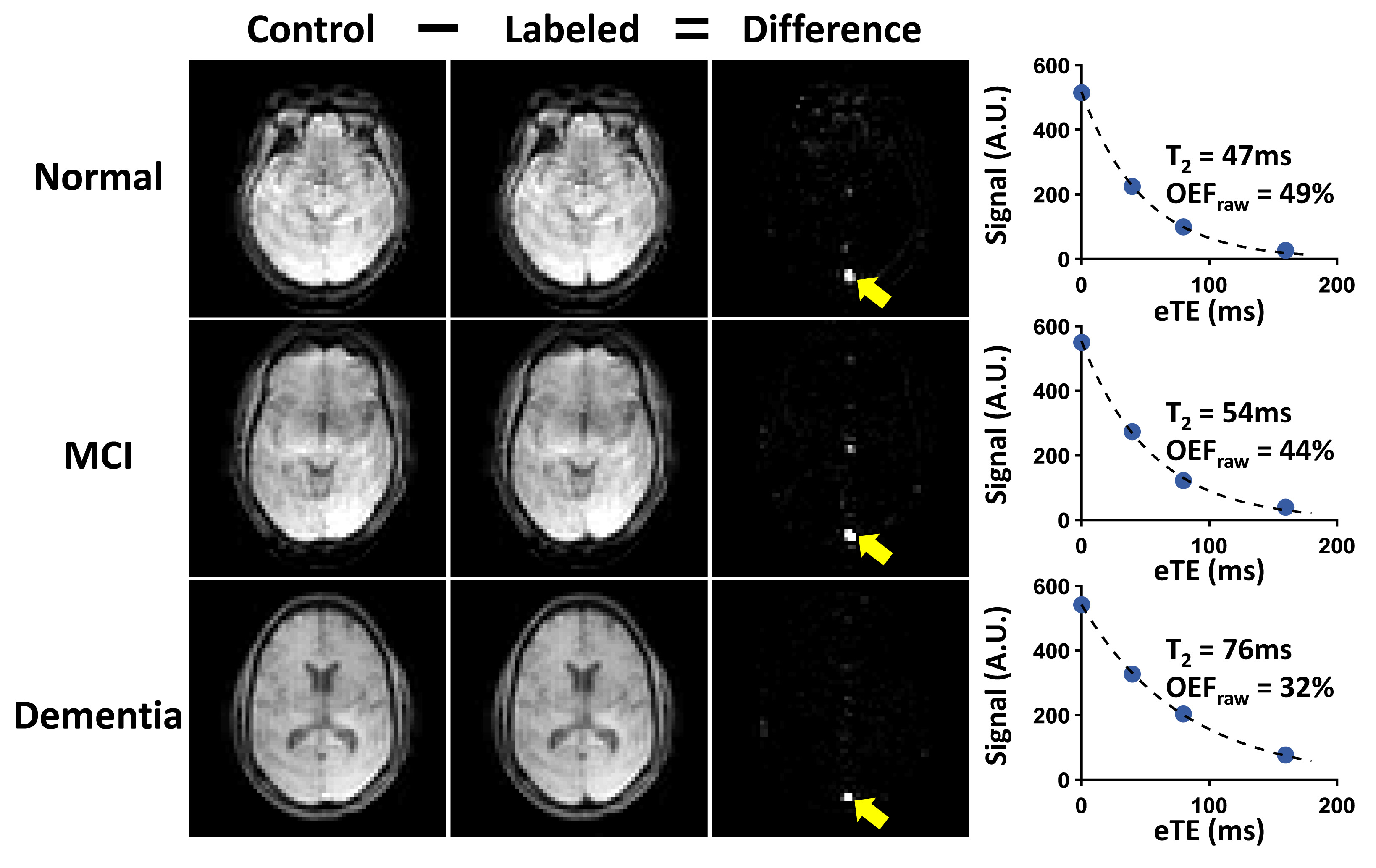
Figure 1. TRUST OEF data of
representative normal (top row), MCI (second row) and demented (bottom row)
subjects. Subtraction between control (first column) and labeled (second row)
images yields strong venous blood signal in the superior sagittal sinus (yellow
arrows) in the difference images (third column). The scatter plots on the far
right show venous signal as a function of effective TE (eTE). Fitted venous
blood T2 and the corresponding OEF values (before correction) are
also shown.
