Md Nasir Uddin1, Abrar Faiyaz2, and Giovanni Schifitto1,3
1Department of Neurology, University of Rochester, Rochester, NY, United States, 2Electrical & Computer Engineering, University of Rochester, Rochester, NY, United States, 3Imaging Sciences, University of Rochester, Rochester, NY, United States
1Department of Neurology, University of Rochester, Rochester, NY, United States, 2Electrical & Computer Engineering, University of Rochester, Rochester, NY, United States, 3Imaging Sciences, University of Rochester, Rochester, NY, United States
Microscopic fractional anisotropy (μFA) provides better sensitivity than conventional FA in white matter in HIV-infected individuals

Figure 3: Comparison of microscopic fractional anisotropy (μFA) in white matter ROIs for HIV- vs. HIV+ cohorts: ROI placements on MNI atlas (top), and Whisker box plots for μmFA (bottom). μFA is decreased significantly (p<0.05) in the HIV+ cohort. SCC: Splenium of the corpus callosum; GCC: Genu of the corpus callosum; BCC: Body of corpus callosum; ALIC: Anterior limbic internal capsule; PLIC: Posterior limbic internal capsule; EC: External capsule; SLF: Superior longitudinal fasciculus; CP: Cerebral Peduncle; ACR: Anterior Corona Radiata; and SCR: Superior Corona Radiata.
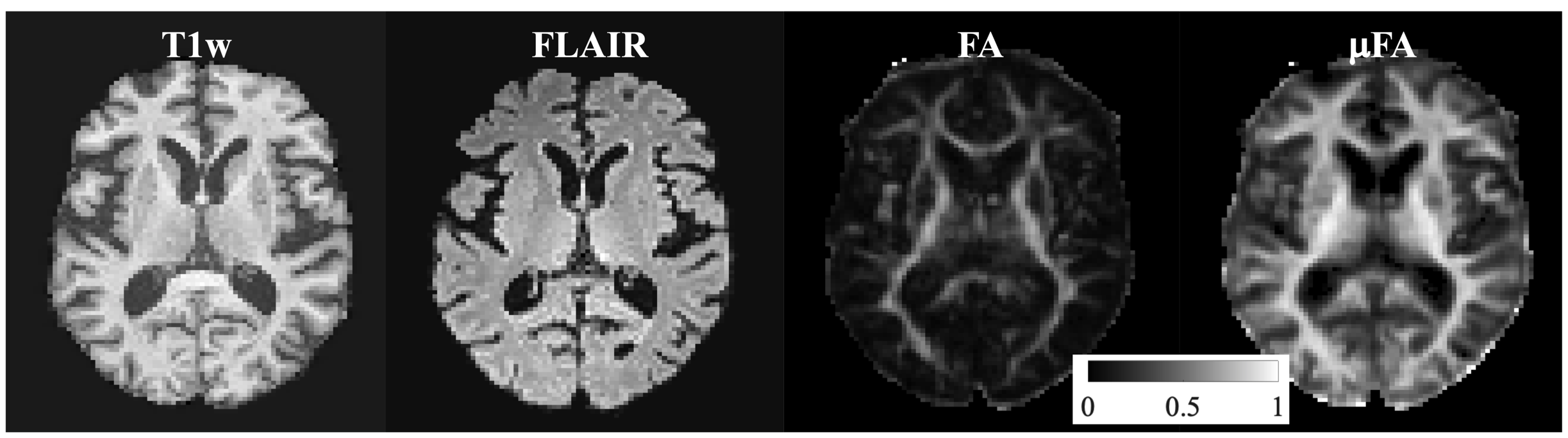
Figure 1: Example axial images from a participant with HIV-infection: T1-weighted (T1w) MPRAGE, T2-weighted (T2w) FLAIR, DTI derived fractional anisotropy (FA) and tensor-valued encoding derived microscopic fractional anisotropy (μFA). The intensity scale for FA and μFA is also shown.
