Rachel W Chan1, Hatef Mehrabian1, Hany Soliman2, Hanbo Chen2, Aimee Theriault2, Sten Myrehaug2, Chia-Lin Tseng2, Jay Detsky2, Wilfred W Lam1, Angus Z Lau1,3, Gregory J Czarnota1,2,3, Arjun Sahgal2, and Greg J Stanisz1,3,4
1Physical Sciences, Sunnybrook Research Institute, Toronto, ON, Canada, 2Department of Radiation Oncology, Sunnybrook Health Sciences Centre, Toronto, ON, Canada, 3Medical Biophysics, Sunnybrook Research Institute, Toronto, ON, Canada, 4Department of Neurosurgery and Pediatric Neurosurgery, Medical University, Lublin, Poland
1Physical Sciences, Sunnybrook Research Institute, Toronto, ON, Canada, 2Department of Radiation Oncology, Sunnybrook Health Sciences Centre, Toronto, ON, Canada, 3Medical Biophysics, Sunnybrook Research Institute, Toronto, ON, Canada, 4Department of Neurosurgery and Pediatric Neurosurgery, Medical University, Lublin, Poland
CEST
at 3T can be used to distinguish between radiation necrosis and tumor
progression after stereotactic radiosurgery. The amide MTR parameter
acquired at 0.52μT was selected from multivariable modelling with an AUC of 0.91.
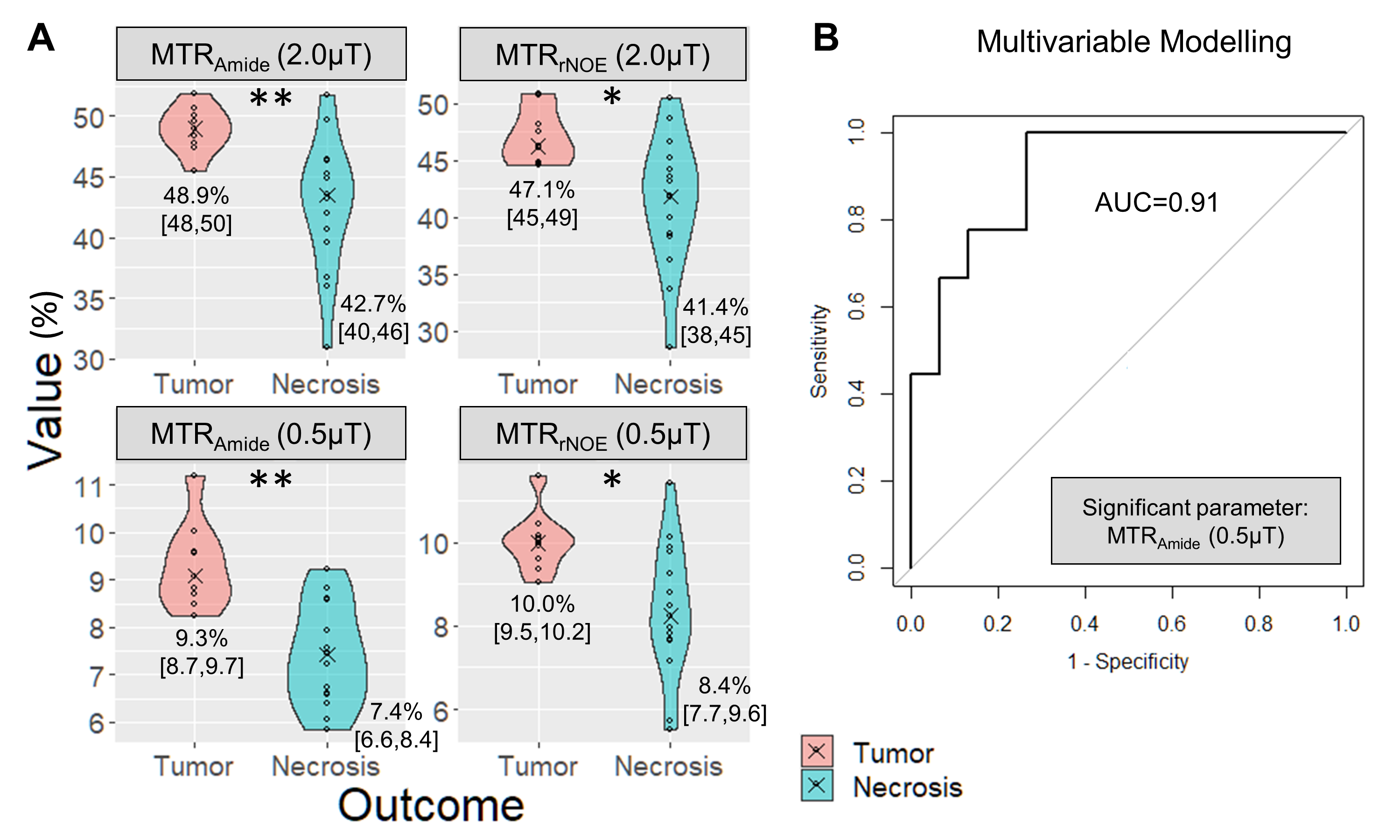
Figure 5 – Tumor and
Radiation Necrosis: (A) The median values with
violin plots are shown for the tumor (red) and radiation necrosis (green)
outcomes. Asterisks represent significant differences (**p<0.01, *p<0.05)
between the two outcome groups after adjusting for multiple testing. (B) The ROC curve is shown of the
significant parameter after multivariable modelling for predicting a tumor
outcome.

Figure 3 – Example of
Radiation Necrosis: The
post-gadolinium T1-weighted images are shown along with the four
CEST maps – MTR amide and rNOE, acquired with B1=0.52μT and B1=2.0μT.
The values on the bottom right represent the ROI medians and standard
deviations.
